ECG's
- ECG Interpretation
- Bradyarrhythmias and Pacemakers
- Supraventricular Arrhythmias
|

|


|

|
|

|
|
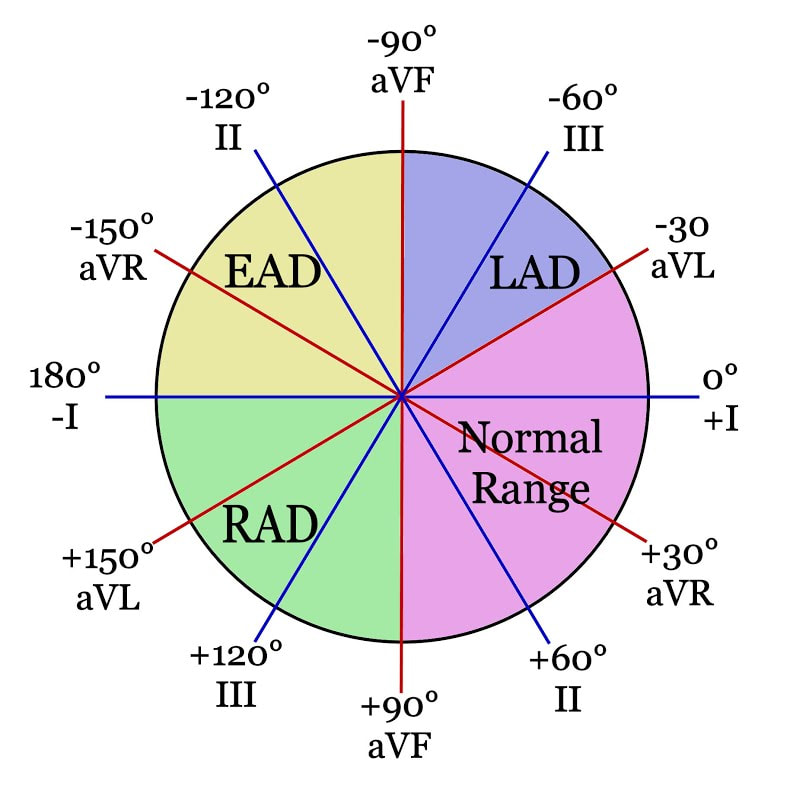
Calculating the Cardiac Axis
|
|
|
Amplitude Changes in an ECG
|

|
|

|
|


|
|
Atrial Hypertrophy
|

|
|

|
|

|
|

|
|

|
|

|

